
OpenMRS is an open source medical records system or EMR with a global community.
The EMR4All Journey: How a Volunteer-Led Mission is Transforming Digital Health in Remote Communities
EMR4All didn’t begin with funding or infrastructure. It began with the question: “Can we run OpenMRS on a Raspberry Pi?”
Figure 1: The first question on Talk by Grace Potma about OpenMRS 3 (O3) on Raspberry Pi, which emphasised the vision of EMR4All in 2023 to become a reality.
It was a technical curiosity that sparked a movement, one driven not by budgets but by belief. The belief that digital health tools should reach even the most remote corners of the world. The belief that skilled volunteers could build solutions where none existed. And the belief that offline, low-cost EMR systems could change lives.
What followed was a grassroots effort fueled by the OpenMRS community, comprising developers, implementers, and advocates who worked together to bring healthcare innovation to places often overlooked by traditional systems.
In just two years, EMR4All has grown from an idea to a field-tested reality. It now powers rural clinics and referral hospitals across countries like Nigeria and the Democratic Republic of Congo. Along the way, it has sparked collaboration, inspired new contributors, and opened doors for other communities to imagine what’s possible.
This is the story of how one question became a breakthrough and how that breakthrough is becoming a movement.
The Challenge
Across many remote and underserved communities, digital health remains out of reach. Clinics and hospitals in these regions often operate without the most basic infrastructure, such as no reliable electricity, no stable internet connection, and certainly no room for expensive, high-maintenance servers.
In these settings, the idea of running a traditional electronic medical record (EMR) system isn’t just impractical, it’s nearly impossible. Even when there’s a desire to digitize patient care, the tools available are often built for environments with far more resources.
As a result, health workers are left without the digital support systems that have become standard elsewhere. Patient records are still kept on paper, reporting is delayed or incomplete, and opportunities for coordination across sites are lost.
This is the gap EMR4All set out to bridge, not with a one-size-fits-all solution but with an approach grounded in reality: offline-first, low-cost, and built for the conditions on the ground.
The Vision Behind EMR4All
The EMR4All project was born from a clear and urgent vision: to bridge the digital divide in patient management for the communities that need it most.
Instead of waiting for better infrastructure to arrive, the team asked, “What if we brought the technology to where people already are?”. That question led to a bold reimagining of OpenMRS: not as a system confined to hospitals with internet and power, but as an offline, portable solution running on compact, low-cost hardware.
At the heart of this vision was the Raspberry Pi, a mini server small enough to fit in a pocket yet powerful enough to run a full EMR system. By adapting OpenMRS to run on this platform, EMR4All unlocked a new kind of access: one that didn’t depend on constant connectivity or complex logistics.
But EMR4All is more than a technical solution. It’s a model for how communities can take ownership of digital health innovation. It’s powered not by contracts but by volunteers working together across borders to bring digital health to the last mile.
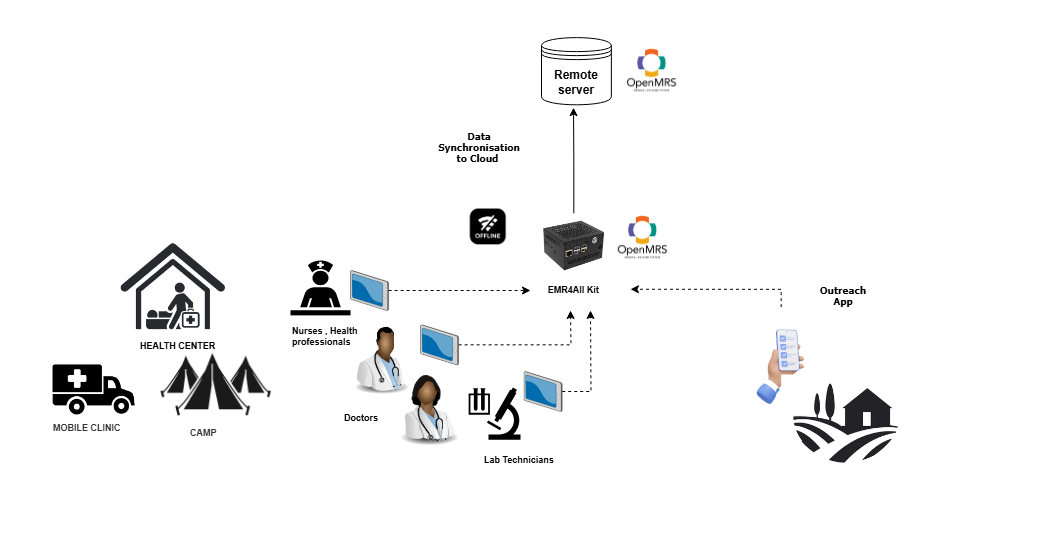
Figure 2: A use case design of the EMR4all kit running OpenMRS offline.
Building a Portable, Offline-First EMR Solution
At the core of EMR4All is a simple but powerful idea: healthcare tools should meet people where they are, not the other way around. That meant building an EMR system that could thrive in conditions where traditional setups would fail. The result is a rugged, portable solution designed specifically for remote care environments.
The Technology Stack
As earlier stated, to reduce the cost and complexity of traditional EMR infrastructure, the EMR4All team turned to the Raspberry Pi. With this mini-server, EMR4All lowered hardware costs by up to 80%, opening doors for facilities that could never afford enterprise-level systems.
The team deployed OpenMRS 3 and Bahmni EMR in an offline-first configuration, enabling full functionality without a constant internet connection EMR4All Kit. Using Docker containers, they packaged the system for fast, modular installation, simplifying setup, updates, and scaling across different sites and contexts.

Figure 3: A presentation of the EMR4All kit component by Benjamin Musole.
Key Features
EMR4All is more than a scaled-down version of existing tools; it also brings new capabilities tailored for frontline care. At its core is an offline AI assistant that allows health workers to query patient data, generate insights, and support clinical decision-making, even without internet access.
The system securely stores patient data locally and synchronizes with central servers when a connection becomes available. This ensures that data is both immediately usable in the field and accessible for national reporting or research.
To support outreach and mobile health programs, EMR4All includes custom modules that adapt the interface and workflows for field teams working in varied, often unpredictable conditions.
System Design for Resilience
In regions where electricity is unreliable or unavailable, EMR4All runs on power banks, enabling continuous operation during outages or mobile deployments. The entire kit is designed to be portable, durable, and easy to use, with built-in local wireless networks and robust onboard storage.
Security is a top priority. EMR4All incorporates SSL encryption, role-based access control, and full compliance with international standards like GDPR. This ensures that sensitive health data remains protected, whether the system is online or offline.
Together, these innovations make EMR4All not just a proof of concept but a viable, scalable solution for digital health in the world’s most underserved places.
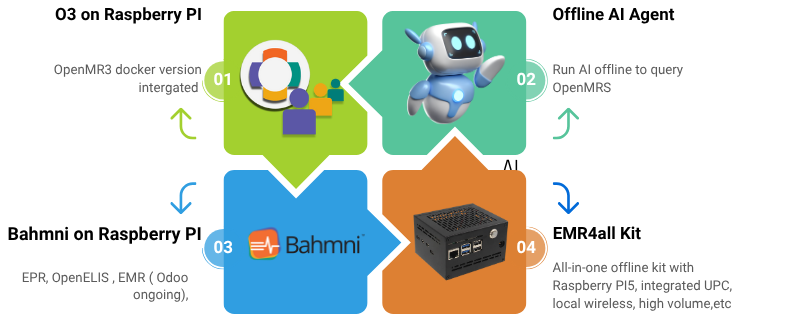
Figure 4: Products delivered by the EMR4All volunteers.
The People Behind the Progress: A Volunteer-Driven Initiative
What makes EMR4All remarkable isn’t just the technology; it’s the people behind it. This project isn’t backed by a large institution or a well-funded startup. It’s powered by volunteers: individuals from across the OpenMRS community who’ve contributed their time, skills, and passion to make digital health work in places where it’s needed most.
The idea for EMR4ALL originated with Mr Benjamin Musole. He wanted to address the issue of inaccessible EMR for distant facilities. Despite lacking funding, he inspired other members of the OpenMRS community to share their thoughts and contribute their skills to bring his vision to life.
Teamwork collaboration
When the project needed to prove its real-world potential, these volunteers stepped up to create demo deployments, showcasing the adaptability of the EMR4All model to local contexts. In a short amount of time, they have taken on demands for the nutrition-specific project in Somalia and built up OpenMRS distribution.
Within approximately two weeks, the team rapidly coordinated, assigned Jira activities and tasks, built system infrastructure and workflow, and set up an AWS instance to address the project’s requirements. For demonstration purposes, the team exceeded the project specifications and successfully deployed a DHIS2 for interoperability with the EMR system. This showcases the proactive involvement of the volunteer teams.
Developer Contributions
From the earliest prototypes to today’s production-ready deployments, developers have been the engine of EMR4All. They built and refined the system’s offline synchronization, AI-powered querying, and mobile-friendly interfaces, ensuring the platform could operate seamlessly in environments without stable connectivity.
They also established GitHub repositories to organize and share code, created developer documentation, and contributed to the wider OpenMRS ecosystem through their work. Their technical efforts have helped EMR4All go from idea to field-ready.
Developer volunteers have demonstrated determination by actively collaborating and offering solutions, including a multi-site synchronization app built in Python. This app pulls data from OpenMRS hosted on a Raspberry Pi and shares it with a remote server. The project was highly appreciated and presented at the OpenMRS conference in 2024 in Kenya, OMRS24: Running OpenMRS on Raspberry Pi.

Figure 5: A presentation of EMR4All at the OpenMRS implementer’s conference, Kenya 2024.
Implementer Impact
While the code made EMR4All possible, implementers made it real. In Nigeria, the team collaborated with local health authorities to launch pilot programs in rural clinics. They configured offline-first installations, provided training to on-site staff, and gathered valuable feedback on usability and system performance.
In the Democratic Republic of Congo, EMR4All partnered with a local organization Afrissol to deploy the system in a French-speaking context including a general referral hospital. Through coordination with local stakeholders, the team ensured that the implementation addressed real needs on the ground and laid the foundation for future scale-up.
These efforts went beyond setup. Implementers customized forms, translated interfaces, and worked hand-in-hand with healthcare workers to ensure the technology fit seamlessly into their workflows.
Advocacy and Community Engagement
Behind every pilot site and new deployment was a network of advocates working to build trust, visibility, and support. EMR4All team members reached out to Ministries of Health, NGOs, and global health organizations, not just to promote the project but to listen, learn, and identify opportunities for meaningful collaboration.
In Uganda, Nigeria and DRC, advocates led efforts to identify new pilot sites and attended national-level meetings for adoption. They represented EMR4All at key events, including the DHIN conference in Nigeria, helping raise awareness about the offline EMR model.
These relationships weren’t just about expanding EMR4All; they helped connect local realities with global digital health strategies, anchoring the project within a larger movement for inclusive, accessible healthcare technology.
Evolving into a Broader OpenMRS Contribution Model
As EMR4All gained traction, something powerful began to take shape: the project wasn’t just improving access to digital health; it was creating a model for community-driven contribution across the OpenMRS ecosystem.
What started as a focused effort to adapt OpenMRS for remote, offline environments has evolved into a broader, more inclusive volunteer program, one that empowers contributors to support OpenMRS as a whole beyond the boundaries of any single initiative.
The Volunteer Program Structure
To sustain this momentum, EMR4All launched a structured volunteer program with three clear tracks: Developer, Implementer, and Advocate. Each track welcomes contributors based on their strengths and interests, offering flexible entry points into the global open-source health community.
But the mission goes beyond building EMR4All. This program is a bridge, linking passionate contributors with opportunities to support the wider OpenMRS platform, especially in areas that benefit multiple projects like offline functionality, data interoperability, and health system integration.
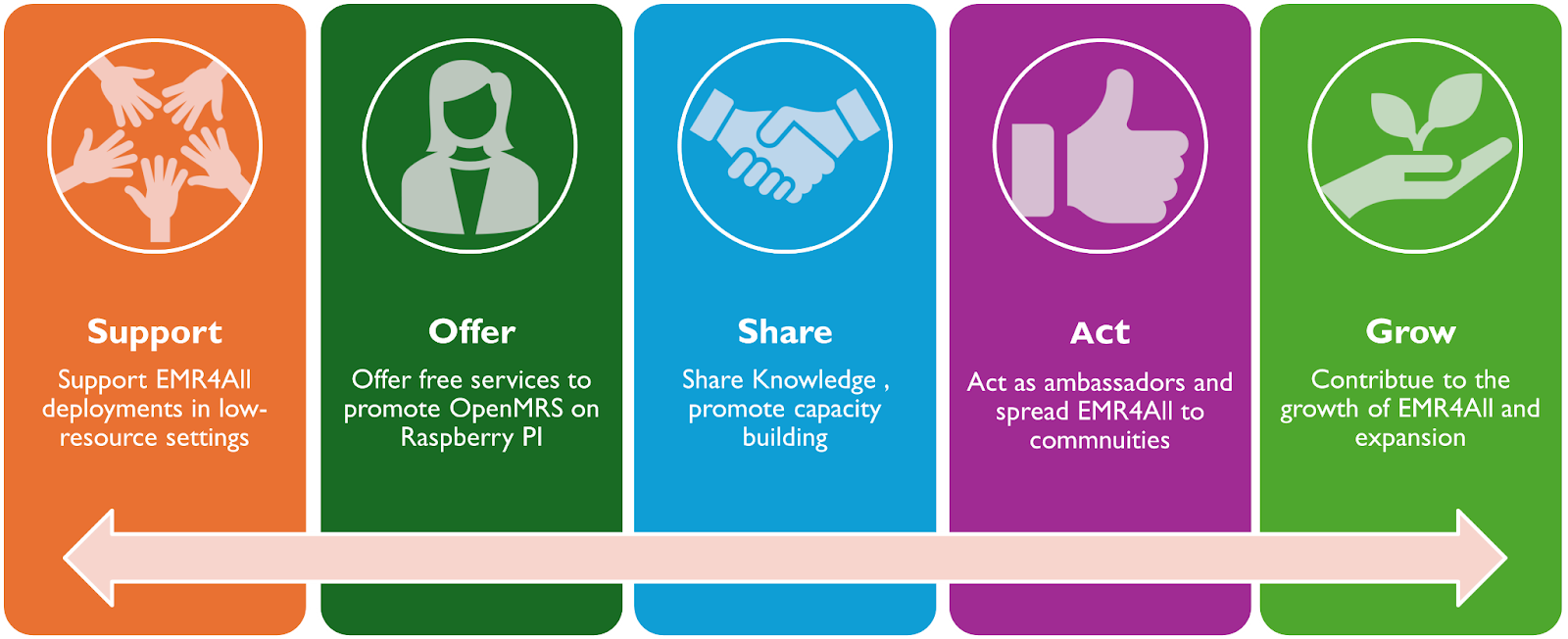
Figure 6: Pillars of the EMR4all volunteers’ driven missions.
How the Program Works
Participation is open to anyone, whether a seasoned contributor or someone completely new to OpenMRS. Once onboarded, volunteers receive a starter guide, join the EMR4All Slack workspace, and are connected to relevant tracks and mentors.
Workflows are centered around curated OpenMRS JIRA tickets, allowing contributors to work on real, needed features with the right level of guidance. Each contribution, be it a bug fix, a new feature, or a documentation update, is part of a larger ecosystem of impact.
To keep contributors engaged, EMR4All has established a recognition system that includes digital certificates, public shout-outs, contributor badges, and even speaking roles at community events. These small but meaningful acknowledgements reinforce the value of every volunteer’s time and talent.
Bridging Projects and Community
By expanding its focus, the EMR4All volunteer program has become a connector, linking individual contributors to broader health challenges and standards. Volunteers are actively customizing OpenMRS features to work offline, not just for EMR4All deployments but for any community that needs it.
This work aligns closely with global health data standards. For example, the team has enabled DHIS2 integration using OpenHIM and built tools for syncing field data to centralized systems, ensuring that even offline clinics can contribute to national health reporting.
Whether it’s improving sync modules, localizing interfaces, or optimizing data flows between facilities, the EMR4All team is helping OpenMRS evolve in ways that support both the community and the countries it serves.
The EMR4All Hackathon: Building Not Just Code, But Change
With its growing community and momentum, EMR4All saw an opportunity to do more than build features, and it set out to build a culture. The EMR4All Hackathon, scheduled this year for July 2025, is not just a coding sprint. It’s a global gathering of minds, talents, and missions aligned around a single goal: to co-create offline-first health solutions that work where infrastructure doesn’t.
What sets this event apart is its intentional structure. Rather than focusing solely on developers, the hackathon welcomes contributors across three tracks, which are Developer, Implementer, and Advocate, ensuring that every angle of digital health transformation is addressed. It’s a sprint rooted in lived realities: clinics without internet, communities without servers, and patients without access to reliable care.
The Event
The EMR4All Hackathon is designed as a multi-day virtual collaboration bringing together participants from around the world. Each track has a specific focus: developers work on adapting and customizing existing OpenMRS features for offline use; implementers develop actionable strategies for deploying these tools in the field; and advocates shape outreach plans for securing partnerships, pilots, and policy support.
Expected Outcomes
The hackathon aims to produce practical, field-ready solutions that can be piloted and scaled. These include improvements to data sync, offline analytics, mobile workflows, and field deployment guidelines, all tailored to the constraints of low-resource environments.
On the implementation and advocacy side, teams will craft strategic rollout plans, develop frameworks for training and support, and build advocacy toolkits to engage ministries of health and global NGOs.
More than the technical output, the hackathon is about growing the community. It will serve as a launchpad for new contributor teams, future project leaders, and long-term champions of offline digital health.
What’s Next: Scaling Up and Sustaining Impact
EMR4All has shown what’s possible when vision, community, and purpose align. But the journey is far from over. With successful pilots underway, a structured volunteer program in motion, and global interest growing, the focus now turns to scaling the work and sustaining the momentum.
Roadmap Highlights
The next phase of EMR4All is about refinement and reach. The team is working closely with pilot sites in Nigeria and the DRC to strengthen feedback loops, ensuring that field realities continue to shape platform evolution.
At the same time, there’s a renewed push to increase visibility and build partnerships with ministries, universities, and global health organizations. These relationships are essential for unlocking new pilots, funding opportunities, and policy alignment.
Equally important is the growth of the volunteer community. EMR4All is investing in mentorship, documentation, and onboarding to help more contributors join and thrive-passing on knowledge, maintaining continuity, and fueling innovation at every level.
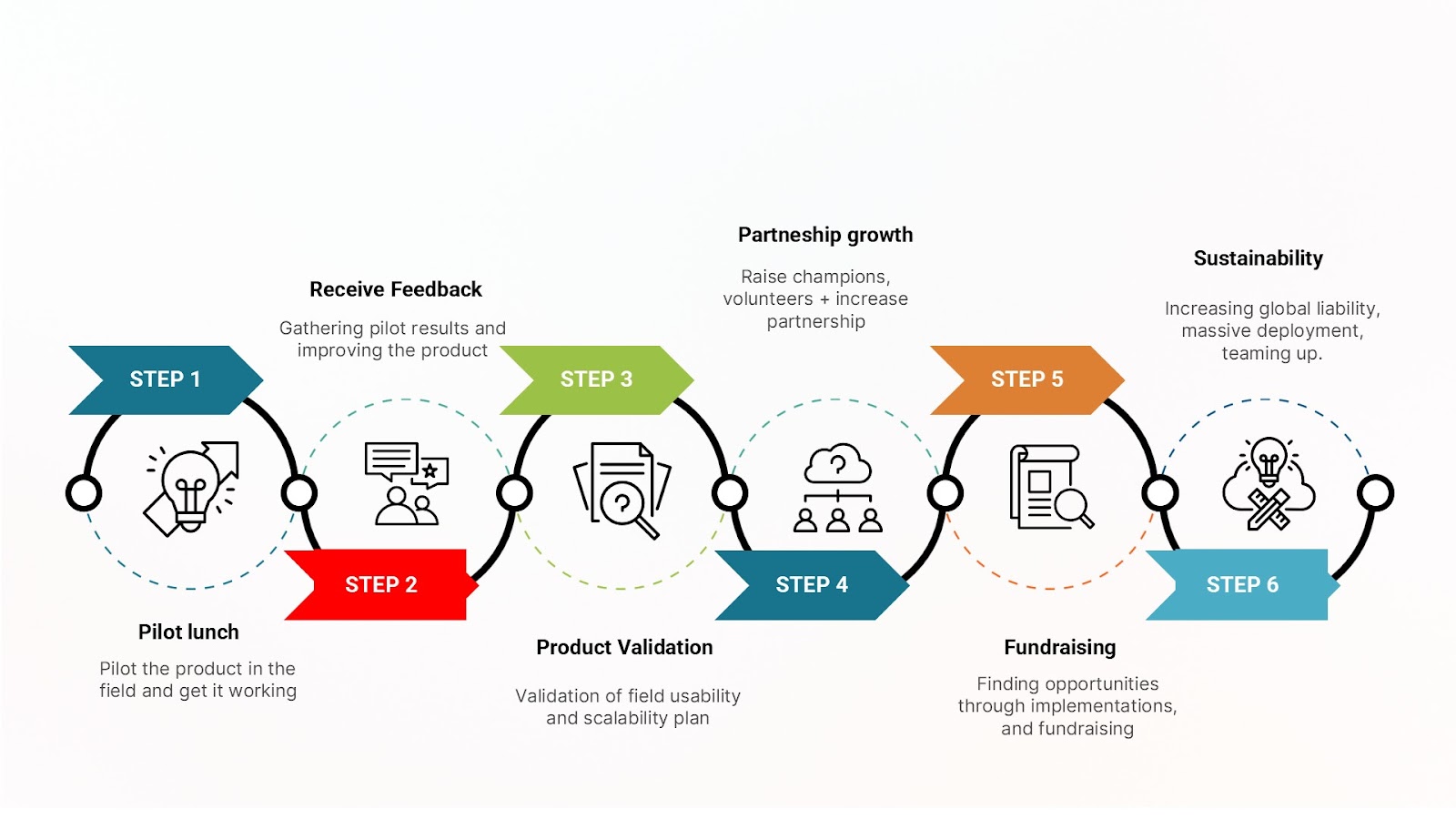
Figure 7: EMR4All scale-up roadmap steps to sustainability.
Call to Action
Whether you’re a developer, health worker, researcher, or advocate, there’s a place for you in the EMR4All story.
- Join the volunteer program and help co-create solutions that work where they’re needed most.
- Support deployments or contribute to documentation, training materials, or strategic outreach.
- Spread the word, attend events, or bring the conversation to your networks.
Stay connected and follow EMR4All through the OpenMRS community, LinkedIn, and X @EMR4All. The story continues, and you can be part of what comes next.